
CHAPTER FOUR: COSTING OF THE NCCEAP
Overview
This section provides a breakdown of the cost estimates for the implementation of the NCCEAP for the planning period 2025–2030. The costs estimates encompass all interventions spent out in the action plan, across the three pillars: expanding HPV vaccination coverage, HPV testing access to PCC treatment, diagnosis and treatment of invasive cervical cancer. A combination of Activity-based costing (ABC) and Ingredients-based costing (IBC) are applied to enable tracking of the individual cost drivers for implementation.
- Any proposed activity, which was deemed to be part of the routine service provision, had no additional costs attached to it. For example, while costs of training and mentorship for healthcare workers are included, their salaries are not. Therefore, the costs represent the additional investment for health system strengthening for an effective cervical cancer response.
- Items with an existing financing mechanism, such as through another domestic source were not costed. For example, the cost of providing HPV testing is included in the Primary Health Care Fund under the Social Health Insurance. Therefore, the cost of offering the service will be eligible when women was not costed separately. However, as estimated the initial cost of availing HPV testing commodities to health facilities countrywide, for them to start offering the service and therefore qualify to be reimbursed under the PHC Fund.
- The implementation of the NCCEAP is premised primarily on domestic financing. Therefore, all effort was made to avoid duplicate costing, since the bulk of the resources will be from domestic public financing.
- The costing exercise was a multi-stakeholder effort, including inputs from the Divisions of Health Financing and Planning (MoH), The Social Health Authority, and accounting officers from counties. Therefore, the cost estimates and resource mobilization strategies proposed are based on in-depth analysis of the current health financing landscape in Kenya.
Financial Resources Requirements
Table 3 shows the breakdown of the cost requirements for implementation of the NCCEAP in the five-year period till 2030. The costs are summarized by pillar, strategic objective and implementation year.
| Pillar | Strategic Objective | 2025/26 | 2026/27 | 2027/28 | 2028/29 | 2029/30 |
|---|---|---|---|---|---|---|
| 1: HPV vaccination | SO1 | 56,721,418 | 56,721,418 | 56,721,418 | 56,721,418 | 56,721,418 |
| SO2 | 1,263,511 | 1,263,511 | 1,263,511 | 1,263,511 | 1,263,511 | |
| SO3 | 0 | 2,432,465 | 2,432,465 | 2,432,465 | 0 | |
| SO4 | 1,597,643 | 1,597,643 | 1,597,643 | 1,597,643 | 1,597,643 | |
| SO5 | 0 | 2,545,386 | 2,545,386 | 2,545,386 | 2,545,386 | |
| SO6 | 0 | 5,771,937 | 5,771,937 | 5,771,937 | 5,771,937 | |
| SO7 | 0 | 18,974,834 | 18,974,834 | 18,974,834 | 18,974,834 | |
| Subtotal | 59,582,572 | 89,307,193 | 89,307,193 | 89,307,193 | 86,874,728 | |
| 2: Screening and PCL treatment | SO1 | 0 | 12,269,134 | 12,269,134 | 0 | 0 |
| SO2 | 0 | 8,023,579 | 8,023,579 | 8,023,579 | 8,023,579 | |
| SO3 | 0 | 29,009,896 | 29,009,896 | 29,009,896 | 29,009,896 | |
| SO4 | 0 | 15,427,920 | 15,427,920 | 15,427,920 | 15,427,920 | |
| SO5 | 0 | 317,153 | 317,153 | 317,153 | 317,153 | |
| SO6 | 0 | 998,877 | 998,877 | 998,877 | 998,877 | |
| SO7 | 8,136,279 | 8,136,279 | 8,136,279 | 8,136,279 | 8,136,279 | |
| SO8 | 0 | 11,905,734 | 11,905,734 | 11,905,734 | 11,905,734 | |
| Subtotal | 8,136,279 | 86,088,572 | 86,088,572 | 73,819,438 | 73,819,438 | |
| GRAND TOTAL | 132,552,273 | 287,792,638 | 277,613,438 | 269,221,577 | 266,789,112 | |
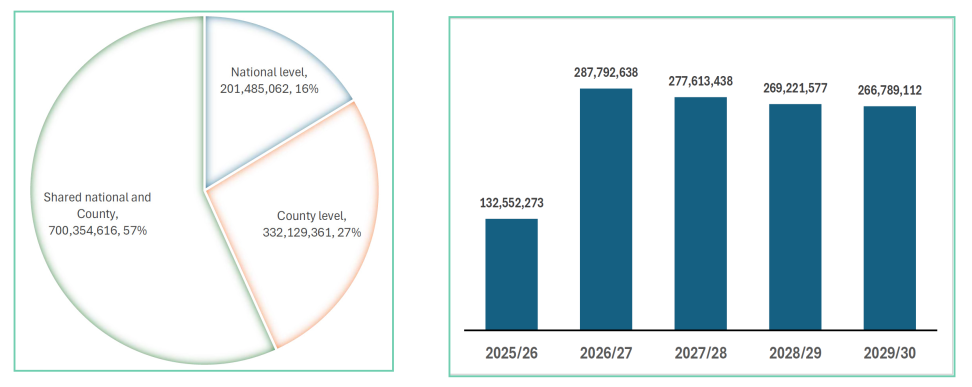
Figure 7: NCCEAP implementation cost by level of government (KES)
Notes
- Additional investments and total cost: In addition to the implementation of the activities in the NCCEAP, expansion of PET/SPECT services by establishing two units (MRI and Mombasa cancer center) is estimated to cost KES 1,389,600,000. Therefore the total cost of implementation would be KES 2,623,569,039.
- Relative cost distribution: The average annual cost of implementing the NCCEAP represents 5.45% of the average cost of implementation of the NCCS 2023–2027, 0.7% of the annual cost of implementation of the NCCS strategic plan 2021–2025 and 0.44% of the total budget allocation to health in the fiscal year 2025/26.
- Cross-cutting benefits: Several investments proposed in the NCCEAP will be utilized beyond cervical cancer. These include diagnostic and treatment facilities. For instance, molecular diagnostic platforms can be utilized for other priority infectious diseases such as TB and HIV.
Resource Mobilization Strategies
1. Government-Led Approaches
- a. Social Impact Bonds (Outcome-Based Funding): Funder pays only after agreed outcomes are achieved (e.g., Tiko, Kiambu Maternal Health). Key Action: Government agencies to sensitize counties and other implementing bodies on the model and its benefits.
- b. Direct Public Funding: Strengthen county and national government participation in the budget-making process. Support policy adjustments (e.g., adopting one-dose cervical cancer vaccine schedule instead of two). Ensure timely remittance of funds to SHA, indigent support programs, and county health accounts.
- c. Operationalization of Laws and Funds: Activate underutilized statutory funds such as the Tobacco Fund and Sports Fund. Key Enabler: Political goodwill and stakeholder advocacy for enforcement.
- d.: Enhance sensitization and capacity-building on PPP frameworks for counties and health facilities.
- e. Equipment Leasing / Fee-for-Service Models: Encourage leasing arrangements and pay-per-use models to ease capital expenditure burden and improve service availability.
- f. Strengthening Social Health Schemes: Introduce levies on selected goods/services to boost SHA resources.
- g. Loans and Grants: Mobilize concessional loans and research grants for cervical cancer elimination programs.
- h. County Government Contributions: Utilize Facility Improvement Funds (FIF) to support local outreach programs, screening initiatives, and Health Products and Technologies (HPTs).
2. Corporate Social Responsibility (CSR)
Engage corporates to fund awareness campaigns, screening drives, and vaccination programs as part of their CSR initiatives.
3. Local Philanthropy
Map and engage local philanthropists to align their giving with national and county cervical cancer elimination priorities.
4. Community Resource Mobilisation
Organize high-visibility fundraising events such as marathons, art auctions, and dinners to rally public support and raise funds.
5. Private Health Insurance Expansion
Advocate for private insurers to expand coverage to include cervical cancer vaccination, screening, and treatment.
6. Development Partners and Civil Society Organizations (CSOs)
Strengthen partnerships for funding, capacity-building, and advocacy support.
7. Unlock Technical Efficiencies
Integrate service delivery across programs to reduce duplication. Automate and digitize processes to save time and costs. Implement pooled procurement to leverage economies of scale. Budget/resource optimization of institutional funding for cervical cancer.
Resource Management
The following measures will ensure prudent and efficient utilization of resources available for CCE in the country:
- Digitisation of Manual Processes: Shift from paper-based systems to electronic data capture and reporting.
- Automation of Processes: Use technology to streamline workflows, approvals, and payments.
- System Optimisation: Improve interoperability between health systems for better data sharing and decision-making.
- Service Integration: Deliver multiple services (e.g., screening, vaccination, treatment) in a single visit to increase efficiency.
- Pooled Procurement: Consolidate purchases across counties and programs to reduce costs.
- Use of AI and Analytics: Apply artificial intelligence for demand forecasting, disease surveillance, and program planning.
- Social Accountability: Engage communities to monitor service delivery and ensure transparency.
- Resource Tracking and Audits: Strengthen financial tracking, audits, and reporting for efficient use of funds.
Risk Analysis and Mitigation Measures
| Risk | Description | Mitigation Measures |
|---|---|---|
| Inadequate Financing | Limited domestic and external funding may delay or scale down implementation of cervical cancer interventions. | Strengthen domestic resource mobilization, expand insurance coverage, and engage development partners and private sector financing. |
| Weak Health System Capacity | Insufficient infrastructure, equipment, and trained workforce to deliver services effectively. | Invest in health workforce training, infrastructure upgrades, and supply chain strengthening. |
| Supply Chain Disruptions | Interruptions in availability of vaccines, screening commodities, and treatment supplies. | Strengthen forecasting, procurement systems, and last-mile distribution mechanisms. |
| Low Community Awareness and Demand | Limited awareness and socio-cultural barriers affecting uptake of services. | Implement targeted communication strategies, community engagement, and behavior change interventions. |
| Data Gaps and Poor Reporting | Inadequate data systems affecting planning, monitoring, and decision-making. | Strengthen health information systems, digitization, and data quality assurance mechanisms. |
| Policy and Governance Challenges | Weak coordination, policy implementation gaps, and limited accountability mechanisms. | Enhance governance structures, coordination platforms, and accountability frameworks at national and county levels. |
