
EPIDEMIOLOGY OF CERVICAL CANCER
Overview
Cervical cancer is a leading cause of disease burden among women in many settings globally. Different populations are affected disproportionately, even in the same country.
Global and Regional Context of Cervical Cancer
Cervical cancer remains a major global public health concern, particularly in low- and middle-income countries. It is the fourth most common cancer among women worldwide, with an estimated 660,000 new cases and 348,000 deaths annually. The disease is primarily caused by persistent infection with high-risk human papillomavirus (HPV) types. Although cervical cancer is largely preventable through HPV vaccination, screening, and treatment of precancerous lesions, gaps in access to these services especially in resource-limited settings continue to drive a high burden of disease and mortality.
Regionally, the burden of cervical cancer shows marked geographic variation reflecting differences in access to prevention, screening, and treatment services. Sub-Saharan Africa, South Asia, and parts of Latin America experience the highest incidence and mortality rates globally. In Sub-Saharan Africa in particular, cervical cancer is often the leading cause of cancer-related death among women, driven by low screening coverage, limited access to HPV vaccination, and weak health system capacity for early diagnosis and treatment. High-income regions such as North America and Western Europe have achieved substantial reductions in both incidence and mortality through the implementation of organized screening programs and widespread HPV immunization. These disparities underscore the critical role of health system strength, resource allocation, and equitable access to preventive and curative services in shaping cervical cancer outcomes across regions.
Cervical cancer disparities are driven by social, economic, and health system inequities, with women from low socioeconomic and marginalized populations experiencing higher incidence and mortality due to limited access to prevention, screening, and treatment. Effective control relies on HPV vaccination, regular screening (preferably HPV testing), and timely treatment of precancerous lesions, though coverage remains uneven in many low-resource settings. Women living with HIV are at significantly higher risk up to six times more likely to develop cervical cancer due to impaired immune response and faster disease progression. Integrating cervical cancer services into HIV care is essential to reduce this disproportionate burden.
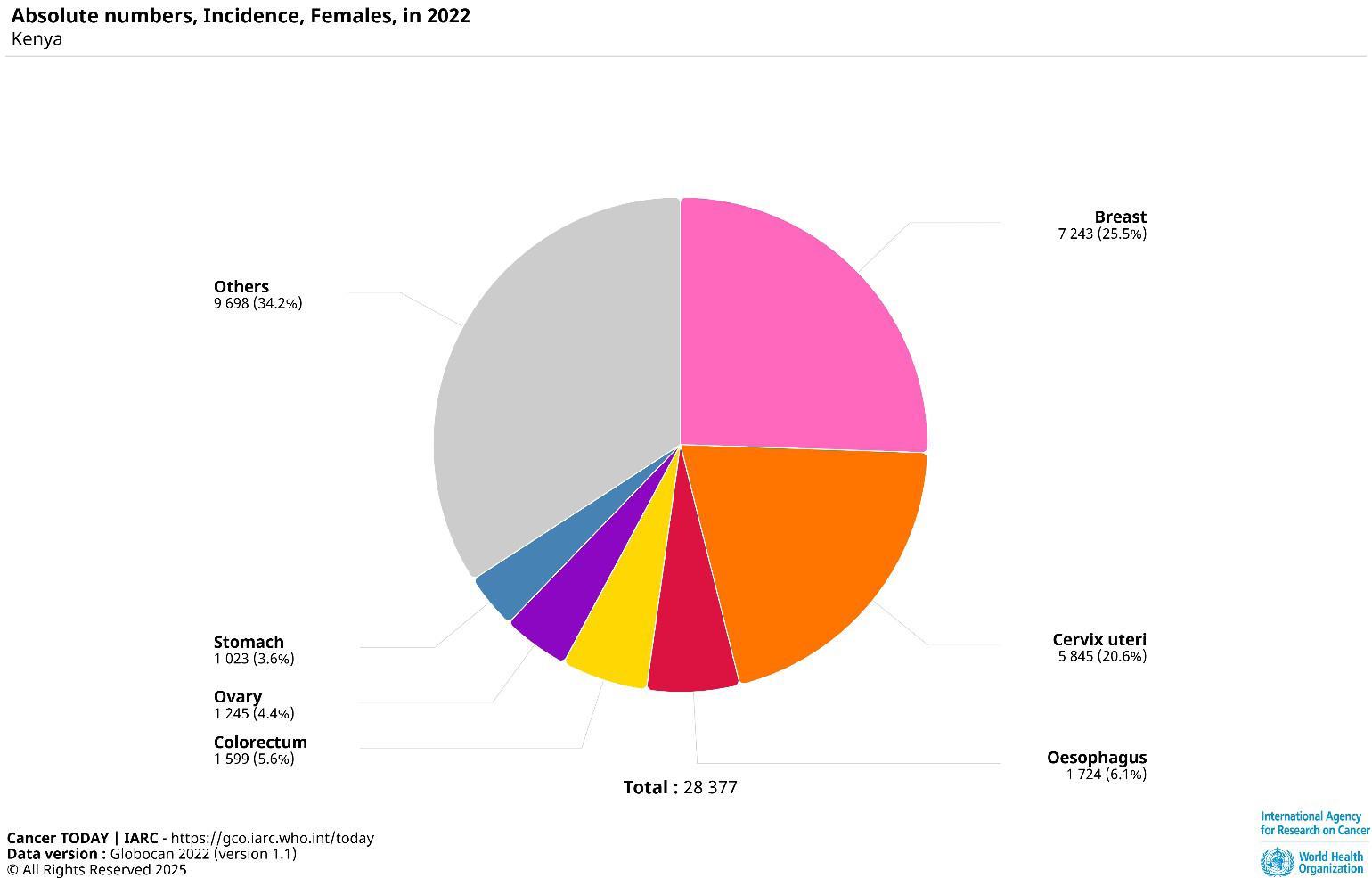
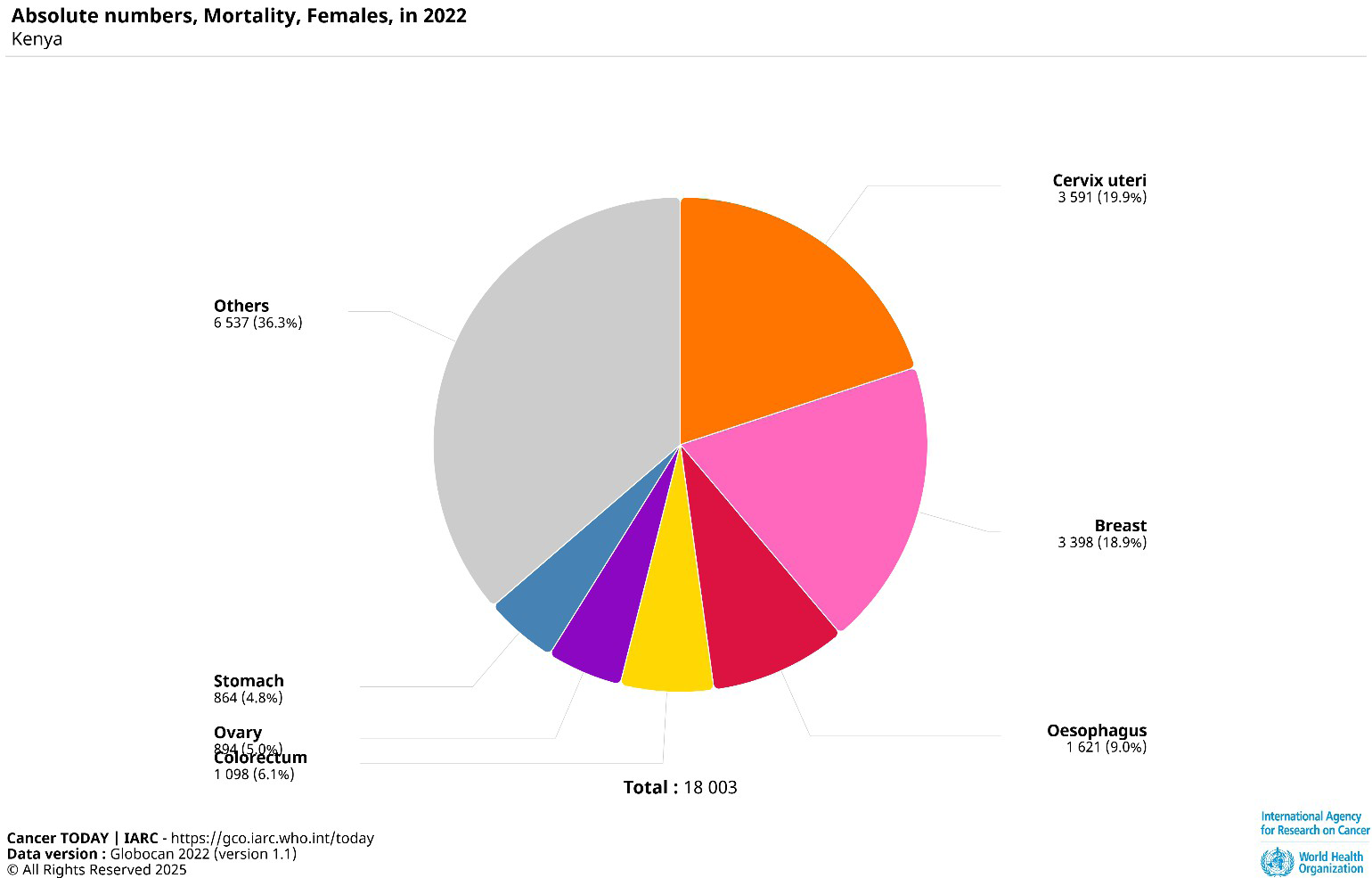
Burden of cervical cancer in Kenya
Women living with HIV are at significantly higher risk of developing cervical cancer due to their compromised immune systems, which make it more difficult to clear high-risk HPV infections the primary cause of cervical cancer.
Global response to cervical cancer: the Global Elimination Initiative
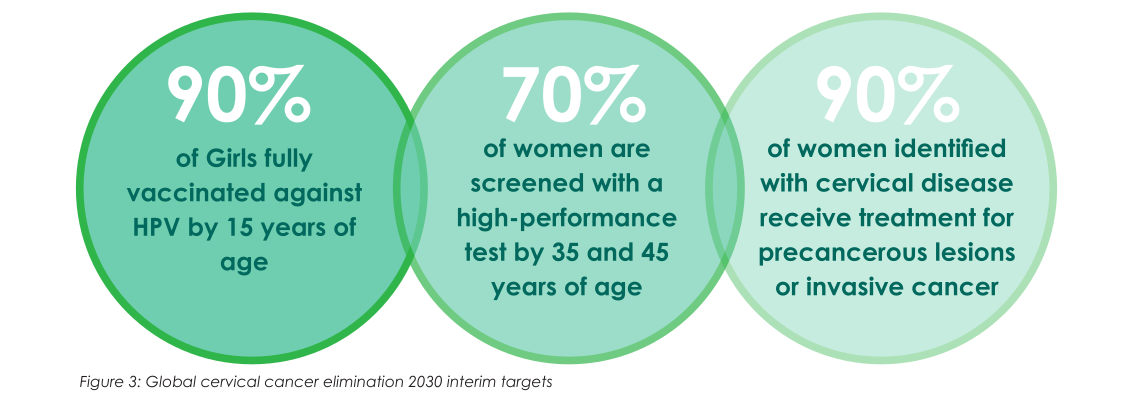
In May 2018, WHO called for the elimination of cervical cancer, resulting in the Cervical Cancer Elimination Initiative and the 2020 Global Strategy aiming to reduce cervical cancer incidence to below 4 cases per 100,000 women by 2030. The targets are 90% of girls fully vaccinated against HPV by age 15, 70% of women screened by ages 35 and 45, and 90% of those with pre-cancer or cancer receiving appropriate treatment.
Achieving these requires political commitment, sustainable financing, community engagement, and integration into existing health systems. The strategy highlights securing affordable vaccines, strengthening delivery and laboratory systems, expanding outreach, addressing social and structural barriers, and ensuring quality, people-centred care.
Justification and process of developing the action plan
Although cervical cancer elimination is included in the National Cancer Control Strategy 2023–2027, a dedicated operational plan was needed to accelerate progress toward the 2030 targets. The National Cervical Cancer Elimination Action Plan (NCCEAP) provides a focused, coordinated, and time-bound roadmap to translate national priorities into concrete actions, clarify stakeholder roles, and align investments across prevention, screening, diagnosis, and treatment.
The plan development started in December 2024 with governance formation, followed by a stakeholder workshop in March 2025 for program performance review, gap and root cause analysis, and priority setting. Subsequent technical workshops developed the draft plan, including costing and advocacy products. After external review and validation, the plan was launched and will be disseminated and implemented nationwide to close gaps and advance cervical cancer elimination.
